
Ending the Medicare Advantage advantage
The outgoing Biden team just proposed MA plans receive an unwarranted 4.3% bump in payments next year. It could get a lot worse with the surgeon turned insurance salesman in charge of CMS.

Late last Friday afternoon (the traditional hour for governments and corporations to release news they don’t want mainstream media to report), the outgoing Biden administration proposed giving private insurance companies a 4.3% pay increase for next year’s Medicare Advantage plans, which now cover more than half of all seniors.
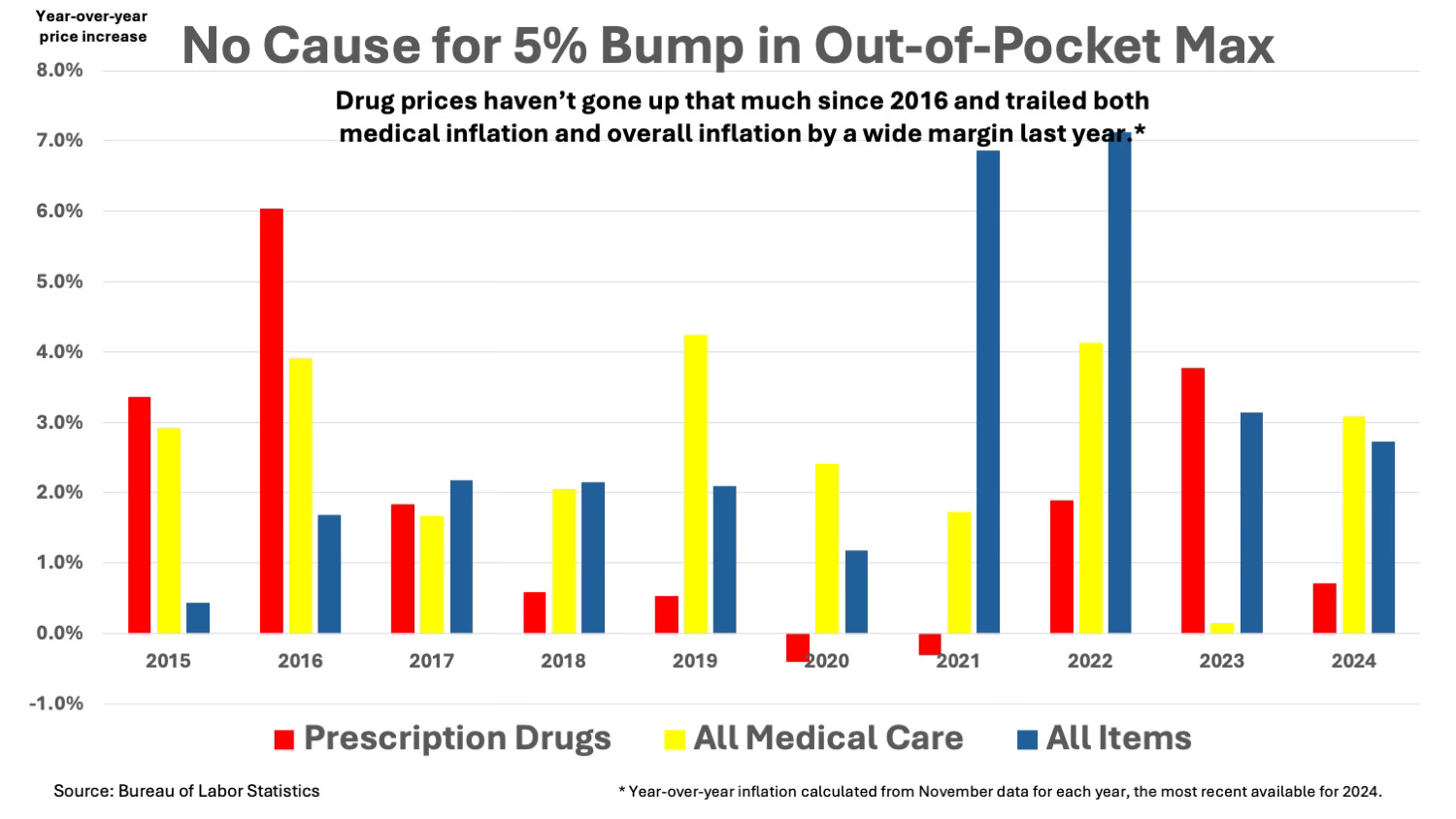
That’s a full percentage point higher than last year’s medical inflation rate and nearly one-and-a-half percentage points higher than general inflation. (See chart.)
The Centers for Medicare and Medicaid Services also proposed a 5% increase in the new cap on out-of-pocket pharmaceutical expenses, raising it to $2,100 in 2026. That is more than five times last year’s drug price inflation rate. Since drug plans are included in 97% of MA plans, it will also lead to a small shift in drug costs from insurers to MA plan members.
The outgoing leadership at CMS called its proposed increases necessary to keep the MA program “stable.” The final determination will be left to the incoming Trump administration, which nominated Dr. Mehmet Oz to run the agency.
Oz, a former heart surgeon, touted MA plans during his 15 years offering medical advice on television. During his unsuccessful 2022 Senate run in Pennsylvania, Oz advocated making MA the near universal program for Medicare beneficiaries.
Stable is one way to describe making no change in the special treatment already given to MA plan insurers. The proposal broke no new ground for closing the $50 billion gap between what plans are paid and what the government would pay if the 37 million seniors in MA were reenrolled in government-run Medicare. CMS pays MA plans an estimated 22% more than traditional Medicare, according to the Medicare Payment Advisory Commission (MedPAC), the Congressionally authorized watchdog.
Let’s put that $50 billion a year in extra payments in perspective. It is more money than the government spends each year on medical research through the National Institutes of Health. It is four times the amount spent each year on public health by the Centers for Disease Control and Prevention. It is eight times the amount spent each year on pandemic preparedness.
It is like dropping bales of dollar bills onto the fires raging in Los Angeles.
Prone to abuse
Medicare pays more for MA plans largely because some insurers engage in rampant upcoding. They use home visits and medical record searches to identify conditions that beneficiaries have but aren’t being treated. MA plans receive extra payments when enrolling these “high risk” patients. Total reimbursement is based on the care beneficiaries received in the previous year with a guess (based on identified conditions) for what people will receive in the coming year.
This process, known as risk adjustment, is common to rate setting for all types of insurance. Life insurers charge smokers more. Car insurers charge people with DUI arrests more.
Risk adjustment is prone to abuse when used in health care because the gap between merely identifying a disease and actually treating it can be quite large. The ten most frequently coded conditions in Medicare include diabetes, chronic obstructive pulmonary disease, heart failure, depression, drug and alcohol abuse, arthritis and morbid obesity.
Undertreatment is common for most of those conditions. Yet MA plans identify these conditions 47% more often among their clientele than seniors who remain in traditional Medicare, where almost all coding is based on treatments delivered, according to new research in Health Affairs.
Insurers also play games to earn extra quality bonuses, another abused facet of the MA program rewards system. They combine the performance of low-quality plans with high-quality plans (often located several states away) when they report quality scores to CMS. It’s like calculating education attainment for a class where a third of kids have straight Ds and two-thirds earn straight As. The combined average (B-) is just high enough to earn quality bonuses for all.
Over the past decade, MedPAC has repeatedly encouraged CMS to address these abuses. It proposed replacing the quality bonus program with budget-neutral incentives (qualities bonuses to high performers would be offset by penalties for poor performers). This is how quality awards are meted out in traditional Medicare. All plans would be evaluated based on local data only.
MedPAC also pleaded with CMS to overhaul its risk-adjustment model. That would require collecting much better data on the actual treatments MA insurers deliver to plan members.
In recent years, CMS has taken a few minor steps to reduce plan overpayments. It imposed a small, across-the-board reduction in scheduled plan payments. That had the perverse effect of penalizing plans that did not engage in upcoding just as much as those who did.
In its 2023 rule, the Biden administration promised to step up its auditing of MA insurer reimbursement claims that were based on diagnoses but weren’t included in patients’ medical records. Given that the existing Risk Adjustment Data Validation (RADV) program hadn’t collected a dime in overpayments since 2006, it’s not surprising CMS estimated that stepped up policing of bogus claims would only recover $4.7 billion over the next decade, less than 10% of one year’s overpayments to MA plans.
Ideas for change
The latest issue of Health Affairs included several studies that offered suggestions for ways to overhaul risk adjustment in Medicare Advantage. The study cited earlier called for eliminating upcoding for the top ten disease states. Prospective reimbursement for those conditions would be based on actual treatments.
Two studies called for adding patient self-assessments to the risk-adjustment formula. “Combining (coding) scores with survey responses were more predictive of health care use,” a team of Brown University researchers found. That would require a redesign of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey to include gathering information on frailty, food insecurity and conditions like depression.
It would also require a far higher participation rate, which has fallen dramatically in both traditional Medicare and MA over the past two decades. Over two-thirds of Medicare beneficiaries filled out CAHPS surveys in 2004, the year MA began its dramatic growth. Last year, less than a third did, according to the CMS-sponsored Health Services Advisory Group.
Dr. Aaron Schwartz, a professor at the University of Pennsylvania medical school and a Veterans Administration physician, offered an entirely new way of conducting risk assessment – one that would provide a tremendous boost to primary care. He would require risk measurement during the annual wellness visit that all Medicare beneficiaries are supposed to get.
The government could create a standardized risk assessment form and pay primary care physicians to collect all the medical history, biometric and laboratory test data needed to create an accurate picture of potential health care needs. This would require making the annual wellness visit mandatory – a good idea in any case.
The government could also randomly assign beneficiaries to plans. “Random auto-assignment ensures that plans receive beneficiaries with the same risk, on average,” Schwartz wrote. Adjustments in succeeding years would be based on actual medical experience, with higher payments going to plans hit with unexpected costs for people who experience unpredictable illnesses.
It's unlikely the incoming Trump administration will adopt any of these proposals, especially if the Senate approves Dr. Oz to run CMS. If the Republican Congress turns Oz’s desire to make MA universal into reality, it could bankrupt the Medicare trust fund much earlier than 2036, its current projected date.
It might also trigger huge cuts in what Medicare covers. Either would be a disaster for the 68 million seniors and disabled individuals who depend on the program for their health care.