


Little value from high-priced cancer care
Sky-high drug prices were supposed to deliver more innovation. That policy failed.

Anyone paying attention to the drug pricing debate over the past few decades has heard Big Pharma’s argument ad nauseum: America’s high drug prices foot the bill for global innovation. If Medicare were to join the rest of the world in negotiating lower prices, innovation would dry up and the latest miracle cures (always on the near horizon) would disappear from view.
No field of medicine has been more prone to this psychological blackmail than cancer care. Desperate patients, their families and the patient advocacy groups that speak in their name (almost all of which receive substantial funding from the pharmaceutical industry) have allowed themselves to be used as an effective roadblock to granting the federal government the right to negotiate lower-priced drugs.
The non-policy has proven extremely costly for U.S. taxpayers, who pick up the tab for Medicare and Medicaid; employers, who pick up about 75% of the cost of private insurance; and privately-insured families, who pick up the rest. Spending on cancer drugs accounted for 37% of the more than $200 billion that the U.S. spent on cancer care in 2020. On a per capita basis, that is more than any other country on earth.
A new study out this week sought an answer to a simple question. Are we getting a bang for all the bucks we spend? Have high prices and a lax regulatory environment, which gives Americans earlier access to the latest innovations in personalized medicine that are coming out of the bio-pharmaceutical industry’s labs (monoclonal antibodies, kinase inhibitors, immune checkpoint inhibitors and the latest new new thing, CAR-T therapy), paid off in better outcomes for the people sick with the more than 100 forms of cancer?
The short answer is no. The study compared cancer spending to cancer outcomes at 22 peer nations in the Organization of Economic Development and Cooperation. The U.S. ranked slightly better than middle-of-the-pack when it came to total deaths from cancer per 100,000 population. U.S. costs, on the other hand, were the highest, although Switzerland, another country that invests heavily in its pharmaceutical industry (Roche and Novartis are among the major players headquartered there), is closing in fast.
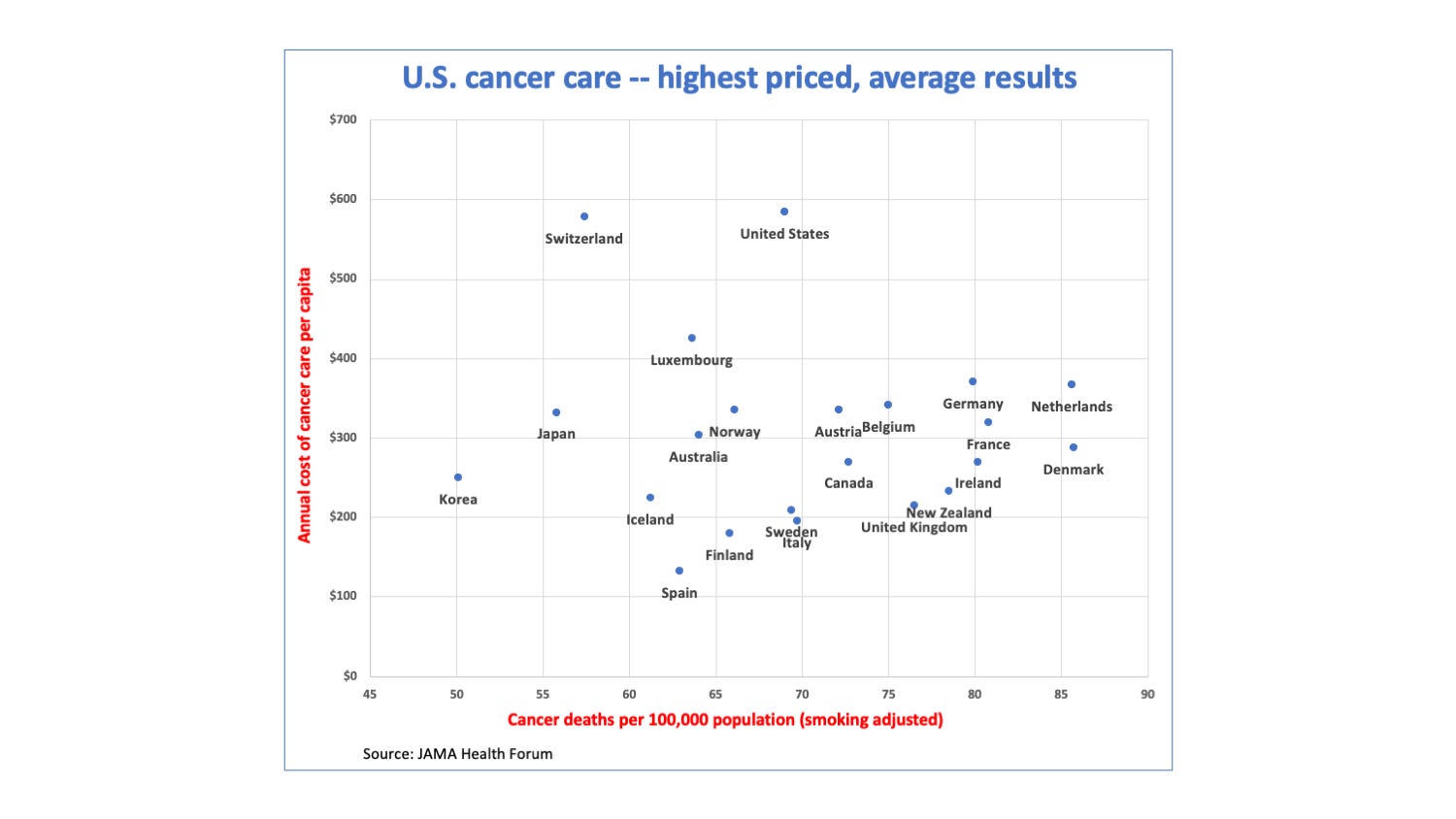
“After adjusting for smoking, nine countries had lower cancer care expenditures and (emphasis added) lower mortality rates than the U.S.,” researchers at the Yale School of Medicine and Vassar College found. “Of the remaining 12 countries, the U.S. additionally spent more than $5 million per averted death relative to 4 countries, and between $1 and $5 million per averted death relative to 8 countries.”
Their bottom line: Cancer care expenditures were not associated with cancer mortality rates. “Much of the growth in U.S. cancer drug spending … often confers marginal or unclear survival gains,” they wrote.
Woodstock for oncologists
The American Society for Clinical Oncology (ASCO) opens its annual meeting in Chicago later this week. Tens of thousands of cancer docs are expected to attend.
A decade ago, I attended these meetings as a freelance writer for the Journal of the National Cancer Institute. I would often find good stories in the studies and abstracts released at the meeting that cast doubt on the high cost and dubious benefits of many of the latest cancer drugs and therapies (including proton beam radiation therapy, whose superior benefits for many of its uses have never been borne out in clinical studies).
Sadly, there is much less of that kind of reporting today. The “hype and hope” public relations machine, which I first wrote about in this 2005 article, grinds on. See, for instance, this more recent article and the list of essays at the end of this article.
Still, Democrats in Congress may yet get their act together this year and pass legislation giving Medicare a limited authority to negotiate over the highest priced drugs, which are often the latest cancer therapies. If they take it up in the Senate, we will no doubt once again be hearing the stale argument that without high prices, there will be no medical innovation.
It simply isn’t true. The limiting factor in achieving medical breakthroughs isn’t money. It’s scientific progress, a process that is inevitably slow and incremental in nature, especially when you’re dealing with a complex disease like cancer. And, it’s most likely to be based on decades of academic research, which is largely funded by the U.S. government, i.e., you and me.
Here’s hoping there is a debate and this Congress actually gets something done before the mid-term elections.
Other recent essays on this topic:
The Cancer Industry: Hype vs. Reality (Scientific American)
Widespread Hype Gives False Hopes to Many Cancer Patients (Kaiser Health News)
Managing Cancer Patients’ Expectations Amid Hype and Hope (Health Affairs)
Is there data shows the number of new cancer drugs and their effectiveness since prices skyrocketed?