


Medicare-for-All-Lite
Two prominent health economists offer a new plan to provide basic health insurance coverage for everyone -- one that will exacerbate existing inequities.

On the wintry day when Barack Obama launched his campaign for president in 2007, the first-term senator promised “universal health care in America by the end of the next president's first term.” In a nation with over 50 million uninsured, providing what every other advanced industrial nation had guaranteed its citizens for over half a century – health insurance for all – seemed long overdue.
Upon taking office, he surrounded himself with centrist health policy advisers who convinced him that insurance reform – getting everyone covered – must be accompanied by delivery system reform to make it affordable. During his predecessor’s eight years in office, health care spending as a share of gross domestic product had soared from 13% to around 17%. With the economy entering a deep recession, it was threatening to rise even higher. The only way to free up tax dollars to cover the uninsured was to bring down costs for the large majority who were already covered.
The 2010 Affordable Care Act, which narrowly passed Congress without a single Republican vote, was designed to achieve both objectives. But the GOP’s intransigent opposition after passage undermined those goals. The Supreme Court gave the green light for states to opt out of Medicaid expansion. A Republican-controlled Congress weakened or eliminated its mandates on employers and individuals. Health care providers and insurers, who had grudgingly endorsed the bill, balked, too. The act’s delivery system reforms never moved beyond the experimental stage.
Despite what journalist Jonathan Cohn’s recent book called “The Ten Year War” against Obamacare, the ACA succeeded in cutting the uninsured rate in half and slowing the growth rate in health care spending. Unfortunately, it left 30 million still uninsured. Meanwhile, the public, policymakers and the press lost interest in the uninsured, turning their attention to the soaring prices and mounting out-of-pocket costs hitting tens of millions of already-insured Americans. Many found themselves with unaffordable bills after becoming seriously ill because they were stuck in high deductible plans or plans with high co-pays for basic services and drugs.
Embracing inequality
With the 2024 presidential campaign looming, the health care policy world will no doubt begin generating new proposals for how to complete the job of insuring all Americans and ending the scourge of rising out-of-pocket costs. A first entry comes from Liran Einav and Amy Finkelstein, economists at Stanford and the Massachusetts Institute of Technology, respectively. In “We’ve Got You Covered: Rebooting American Health Care,” published last month by Penguin Random House, the economists, who specialize in health insurance, propose the creation of a universal, government-funded health plan that covers basic services without premiums, co-pays or deductibles. Call it Medicare-for-All-Lite (they don’t, but that is what it amounts to). Individuals and families would have the option of buying supplemental private insurance coverage for benefits beyond the basic plan.
Before getting into the details of how their proposal would work and how, crucially, its limited coverage would be determined and financed, the authors spend the first half of the book revisiting the well-known failures of the existing insurance system. Its cardinal sin, they write, is fragmentation. We have separate systems to cover the old and disabled (Medicare); the poor (Medicaid); veterans (the VA); workers and their families (employer-based and group private insurance); and the self-employed and people whose employers don’t provide coverage (individual private insurance). Each has its own coverage rules, out-of-pocket expenses, and prices paid to providers.
Beyond the enormous cost of administering such complexity, its fragmentation leads to coverage gaps when people switch jobs or become unemployed. The constant shifting between private plans and between Medicaid and private insurance leaves many people uninsured even when they qualify for coverage. It leads to unfair differences in access to care. The 50 state Medicaid agencies have different rules for who qualifies and what is covered. Employer-provided and exchange-purchased private insurance plans impose sometimes large and varying out-of-pocket costs. Those, in turn, have triggered an avalanche of unpaid medical bills among less-well-off Americans, 37% of whom say they cannot afford a $400 unexpected expense. When COVID-19 struck, collection agencies held $140 billion in debt owed by the un- and under-insured, more than all other forms of consumer debt combined. “The uncertain nature of health insurance coverage,” Einav and Finkelstein write, “is the key to understanding the deep-rooted rot at the core of our health insurance house.”
They reject adding another patch to this inadequate quilt. It’s time to tear down the old system and start anew, they write. But in calling for a single, taxpayer-financed plan without out-of-pocket expenses, they reject creating a comprehensive single-payer plan modeled on Medicare, which covers virtually every medical service available in the health care marketplace, albeit with premiums, co-pays and deductibles. Their basic coverage would be far more limited. Those who want a plan with expansive benefits can buy supplemental insurance – if they can afford it. “Our social contract is to provide a standard of adequacy for health-care needs, not to strive for equality in health or in health care,” they write.
They arrive at their anti-egalitarian premise by tracing the history of insurance provision in the U.S., beginning with Alexander Hamilton’s plan, adopted by Congress in 1798, to tax commercial shipping and fishing vessels to pay for the care of sick sailors dumped in the communities where they made port. The practice overwhelmed local health care providers, which in those days amounted to not much more than the first charity hospitals. Those organizations needed money to house and feed sick sailors far from home and family.
Each additional layer of coverage, beginning with the creation of workers compensation programs in the early 20th century and running through Obamacare, was designed to cover the illnesses of similarly “deserving” groups who didn’t have the money to pay for care – those injured on the job, the old, the disabled, the poor, and the employed but still uninsured. The government added a different program for each whenever that group’s health care needs threatened to outstrip providers’ ability to offer charity care.
They draw up their limited social contract from this questionable reading of history, which ignores the moral imperative of providing equal access to health care for all. Only some minimal but adequate level of care – not necessarily the best care – should be provided to all citizens. It was well expressed in one of the book’s chapter titles: “Adequacy, not Equality.” Can this really be what Franklin D. Roosevelt meant in 1944 when he included health care on his list of basic human rights? Or what Martin Luther King meant when he declared “of all the forms of inequality, injustice in health is the most shocking and inhuman”?
Einav and Finkelstein’s idea that adequacy, not equality of access, is sufficient might find purchase with conservatives and some health care economists. But it’s hard to imagine many liberals embracing this notion.
Rejecting jerry-rigged financing
Yet it was a Democratic Congress under a Republican president that enshrined the principle of adequacy into law. In 1986 President Ronald Reagan signed the Emergency Medical Treatment and Labor Act, which required any hospital taking federal funds to provide immediate care to anyone who showed up in its emergency room, the present day version of the charity ward. The government and private sector providers then built a jerry-rigged funding scheme to pay for the uncompensated care hospitals deliver.
It includes programs that offer special payments to hospitals that serve a disproportionate share of the poor and uninsured, so-called safety net hospitals. The government funnels additional subsidies through the drug reimbursement system (the 340B program, where hospitals and clinics serving the poor pay drug companies Medicaid prices for drugs but get reimbursed by the federal government at the far higher commercial prices).
Paying for the uninsured also relies on cross-subsidization. The higher prices paid by the privately insured cover some of the unreimbursed costs of treating the poor and uninsured. Rejecting these financial subterfuges, the authors approvingly quote several conservative scholars, including Friedrich A. Hayek, the anti-Keynesian Austrian scholar, who argue that a basic (“adequate”) and compulsory universal insurance program to end uncompensated care would make far more economic sense.
Einav and Finkelstein are not obtuse. They recognize there are vast disparities in health outcomes in the U.S.; that life expectancy is lower and illness incidence higher among those with less education, income, and social status; that the largest disparities are found among minority groups, especially African Americans, who in addition to being disproportionately poorer must live with the health-destroying stress of structural racism, what is sometimes referred to popularly as living while Black.
But health insurance is not “the lever to lean on” to end those disparities, they argue. Income and wealth inequality, housing inadequacy, food insecurity, environmental racism, and the other social factors that drive ill-health are best addressed by programs that directly address those inequities, not through the band aids that health care provides. Access to the best health care money can buy is responsible for only a tiny sliver of the difference in outcomes experienced by rich and poor, Black and white, the well- and poorly-educated.
While that is demonstrably true, and the authors cite several studies documenting the case, that does not prove their argument that “as long as the government has fulfilled the social contract to provide access to necessary medical care, health inequality is not synonymous with inequity or injustice.” As they walk readers through their proposed design for a two-tiered health care system in the second half of the book, that is precisely what they describe: a system that will inevitably generate inequities and injustice.
A shack, not a chateau
Let’s start with the positive aspects of their basic plan. There are no eligibility requirements; everyone is automatically enrolled – like Medicare. It is taxpayer financed – again, like Medicare. It is free at the point of service. This mirrors the British National Health Service, not Medicare, where, unless you purchase a comprehensive supplemental plan, you have to pay premiums and co-pays for physician coverage and a deductible before hospital coverage kicks in. They correctly point out that upfront co-pays and deductibles are an ineffective way to limit demand. Countries that have recently imposed them (Germany and France, for instance) quickly realized they save much less than expected (“The juice wasn’t worth the squeeze,” they write. The book is filled with many such tired clichés). And, finally, it covers everyone, thus relieving employers of the responsibility and cost for providing basic health care coverage.
When Einav and Finkelstein turn to addressing the tricky issue of what will be covered by the basic plan, they approvingly call for “a shack, not a chateau.” If you want avocado toast in the morning in your single-bed hospital room, the basic plan won’t be enough for you. (I lost track of the number of times they cited generous hospital amenities as an excludable benefit, even though I’m not aware of any study suggesting they are a significant contributor to America’s outlier status in total cost of care.)
Since the national basic plan will be put on a strict budget to control costs (I’ll turn to this issue in a moment), wait time for services will be inevitable. We may see the return of multi-bed wards. People in the U.S. already wait for appointments, they argue. If it gets out of hand, those times can be regulated, as Congress recently did to reduce wait times at the VA.
Yet in describing what will be covered by the basic plan, they offer a comprehensive menu: primary, preventive and specialist care in physician-run settings; outpatient, emergency room in-patient care in hospital settings. Excluded? That would be a political choice from what they call “the gray area” of health care: infertility treatments, dental and vision care, physical therapy, long-term care and the like. They fail to address what might happen to highly contentious coverage areas like reproductive health and abortion, behavioral health, and substance abuse treatment when the “gray” areas are left to the vagaries of the political process.
Then there’s the equally gray area of what tests, drugs and procedures will be covered by the basic plan; and, when they are, under what circumstances they will be authorized. What is discretionary and what is necessary? The current statutory standard for Medicare coverage is “reasonable and necessary,” which under current legal interpretations is almost everything.
And who will decide whether a new cancer drug should be covered if it costs $250,000 a year and extends life expectancy for someone with stage 4 cancer on average from 24 months to 26 months? Here they endorse the gatekeeping function already deployed by private insurers as a curb on paying for whatever doctors prescribe under fee-for-service medicine.
How will the new plan’s gatekeepers make those determinations? The authors call for committees made up of technocrats and doctors to evaluate the cost-effectiveness of various technologies, especially new and wildly expensive ones. Plan managers would then use that information to inform coverage decisions. This is precisely what Great Britain’s National Institute for Health and Care Excellence (NICE) does for its National Health Service and similar bodies perform in other western European countries.
Remember Sarah Palin’s cry of “death panels”? Such sentiments are not limited to the U.S. There’s been patient pushback in almost every country that deploys cost-effectiveness analysis (CEA) to limit treatment. In the U.S., nascent efforts to deploy CEA through the Boston-based Institute for Clinical and Economic Review have been limited by the ACA’s ban on using the tool in making determinations. Given the political clout of the pharmaceutical and medical device industries; the control physician specialist societies exert over clinical practice; and industry’s proven ability to amplify patient advocacy groups’ voices when they demand access to the latest technologies no matter what the medical science says about their effectiveness; it will be a heavy lift to empower a government-run basic plan to make choices based on CEA.
Price controls off the table
After endorsing the decidedly non-market use of cost-effectiveness to limit choices, the authors re-don their economist hats to reject any form of price controls, even though reasonable prices will be necessary if their new plan is to deliver an adequate level of basic services under the capped budgets they propose. “There’s a large body of evidence that when physicians are paid less, patients get less care,” Einav and Finkelstein write. “And when drug prices are lower, fewer new drugs are developed.”
Einav and Finkelstein spent a lot of time researching health care in other countries. Yet they have nothing to say about average physician pay in the U.S. that is twice as high as other advanced countries, even though there is little difference in the amount of care delivered. They make no attempt to sift the evidence behind the drug industry’s claim that lower prices will harm innovation, which is based on industry-funded studies and has been debunked many times in the medical literature. Indeed, the Congressional Budget Office’s analysis of Medicare’s new drug price negotiations authority estimated it would have almost no impact on new drug development.
Perhaps they’re bowing to political reality. We’ve already seen the drug industry’s response to Congress’ first-ever attempt to negotiate lower drug prices, passed as part of the Inflation Control Act. PhRMA and a half dozen companies have filed suit challenging the program and are threatening to tie it up in the courts for years. Whatever their reasons, the authors ignore the monopolistic stranglehold that hospitals, Big Pharma and the physician guilds have over the current price-setting system, which would seem to be a fitting subject for two health care economists.
They are equally dismissive of two other “cut-waste-quick” schemes: lowering administrative costs and eliminating waste in the delivery system. The arguments they make in each case contradict one another. Medicare has lower administrative costs than private insurance because Medicare does nothing to manage care, they write. Gatekeepers cost money, and their deployment by private insurance companies may help reduce waste “by making patients and their doctors think twice before ordering expensive and potentially unwarranted medical care.”
But then they turn around and say making waste-cutting a central part of their insurance scheme makes no sense. Why? “The tools we have at our disposal tend to throw the baby out with the bathwater—cutting high-value and low-value care alike.” Moreover, it reduces patient satisfaction. Better to take small steps in cutting waste even though “a dozen such repairs would make scarcely a dent in the $4 trillion annual health-care spending.”
Given their abdication on cost control (“universal coverage can – and should – be separated from health-care delivery reform,” they declare), Einav and Finkelstein are forced to admit their basic plan will be a step down in basic coverage for most Americans. “Not in what is covered,” they write, conveniently forgetting their previous endorsement of cost-effectiveness analysis, “but covered care would likely come with longer waits for doctor appointments, more patients in a hospital room, worse hospital food and temperature control, and more hoops to jump through to see a specialist or get the treatment of the patient’s (or their doctor’s) choice.”
The coup-de-grace to the political viability of the Einav-Finkelstein plan is their prescription for a supplemental insurance program that will allow those who can afford it to buy their way out of the bare-bones system they envision. They tout the design, used in some countries, where supplemental coverage pays only the incremental cost of better care and a better patient experience. Supplemental plan purchasers could use the lower payments from the basic plan as a voucher. They tout Medicare Advantage as a potential model for how supplemental insurance could be structured, conveniently ignoring how the privatized version of Medicare uses narrow provider networks, prior authorization controls and retention of at least some of Medicare’s co-pays and deductibles to control costs. Most of the seniors who choose MA do so because it has no upfront premiums.
Losing what you have
It's hard to imagine that the 160 million Americans with employment-based health insurance will willingly embrace getting thrown into a national plan that relies on purchasing additional coverage to retain what they have, especially if they are in “preferred provider” plan that does not have limited networks. Sure, some generous employers will continue to provide and pay for comprehensive supplemental plans. But most will offer a range of plans, as they do now, with varying limits and out-of-pocket costs. Some portion of the public, especially those on fixed or modest budgets, will forgo supplemental coverage to save money. Some will choose high deductibles and co-pays in their supplemental plans to lower their premiums. The end result will be the same variable priced and hassle-producing system we have now.
Einav and Finkelstein might protest that I’ve been too harsh in describing their basic plan as bare bones. I would simply point to their book’s only discussion about how to finance it, contained in a scant three paragraphs in a chapter entitled Budget Matters. They point out that U.S. taxpayers already pay about 8 to 9 percent of GDP for Medicare, Medicaid, the VA and a few other federal and state-financed health care programs, which is about the same as the UK, Canada and Germany. “Taxpayer-financed health-care spending in the U.S. is already large enough to pay for universal basic coverage,” they assert.
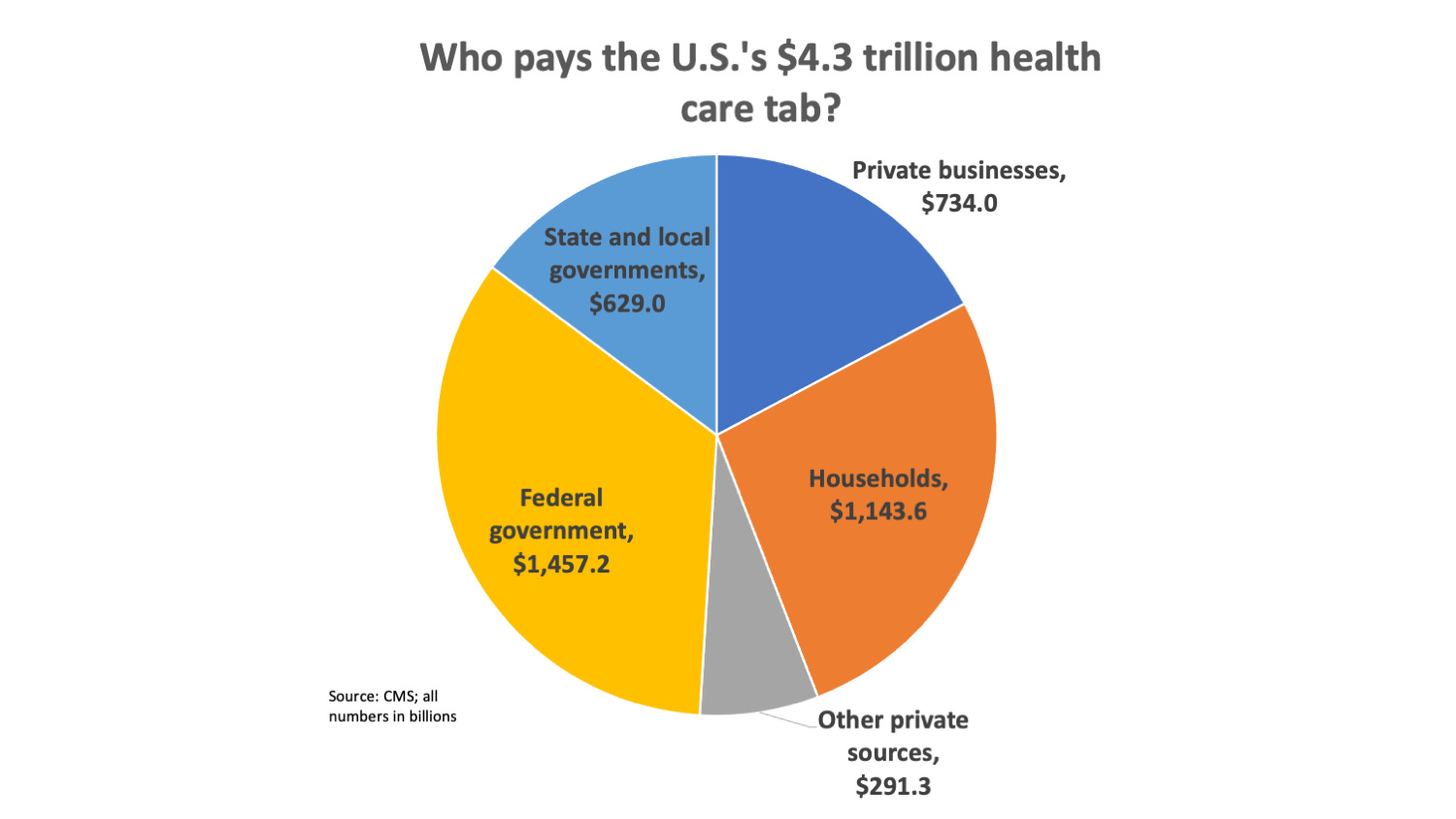
They forgot to mention that American taxpayers are only paying for the old, the poor and less well-off, some veterans, some children and the disabled. Businesses and households are paying for the other half of the population — the aforementioned 160 million privately-insured. The income tax exclusion subsidizes only a third of the $750 billion businesses provide in health care benefits. If everyone were put in the basic plan (even at Medicare prices, which providers will vociferously oppose as they did in Washington State when it set up a public option on its exchange), then taxpayers are going to have to pay more – a lot more. That requires capturing some portion of the nearly $2 trillion paid by businesses and householders.
In other words, creating a government-funded, single-payer, uniform insurance plan – whether it is Bernie Sanders’ Medicare-for-All or Einav-Finkelstein’s Medicare-for-All-Lite — requires comprehensive tax reform. As anyone on Capitol Hill can tell you, that is as heavy a lift as comprehensive health care reform. Vermont’s liberal governor scuttled the nation’s only attempt to enact a state-based single-payer health insurance system after learning the level of taxation needed to finance it. Even a very limited version of Medicare-for-All-Lite would require some measure of tax reform.
Let’s suppose for the moment that political circumstances changed and a majority in Congress opted for comprehensive reform along the lines proposed in “We’ve Got You Covered.” The system’s taxpayer-financed basic plan would be permanently vulnerable to the whims of politics. Look no farther than what has happened to Great Britain’s much-beloved National Health Service in the decade after uniformed doctors and nurses marched in the opening ceremony of the 2012 London Olympics. A series of Tory governments repeatedly slashed the NHS budget, triggering the greatest crisis in its 75-year history. Britains marked its anniversary last month with physician strikes, complaints about the longest wait times ever, and a spate of articles lamenting the state of both the service and its de-spirited workforce.
I cannot imagine many Democrats or Republicans signing onto Einav-Finkelstein program. Polling that took place just before the pandemic on how to achieve universal coverage showed nearly three-quarters of the public favored either Medicare-for-All or a public option offered on the Obamacare exchanges. Any candidate offering Medicare-for-All-Lite won’t put much of a dent in those numbers. If some think tank, policy entrepreneur or academic has a better way to reach acceptable universal coverage at an affordable price, the nation’s in-box remains wide open.