


One other good idea from RFK Jr.: Boost primary care
While public health advocates are mobilizing to thwart the anti-vaxxer's confirmation, his acolytes want to revamp physician pay to boost primary care. It's long overdue.

Robert F. Kennedy Jr. is brimming with wacky and potentially dangerous ideas, but some are not. For instance, the 70-year-old’s focus on the health harms caused by processed foods and environmental toxins draws praise from across the political spectrum, including Senator Bernie Sanders of Vermont.
Here’s another one that stands out as eminently sensible and long overdue. Donald Trump’s nominee to head the Department of Health and Human Services says he wants to change how Medicare compensates physicians. The current system overcompensates specialists and underpays primary care physicians.
The government program and private payers offer exorbitant salaries to those who replace knees and hips, clean out clogged arteries, and administer complex cancer chemotherapy regimens. At the same time, the healthcare system shortchanges the primary care docs who promote prevention and wellness, manage patients with multiple chronic conditions, and daily see people with symptoms of unknown origin.
Those compensation priorities are set by a little-known committee of the physicians’ lobby, the American Medical Association, which, despite its outsized clout, represents just one in five physicians today. Each year, its Relative Value Scale Update Committee (RUC), whose membership is dominated by highly paid specialists, recommends what the Centers for Medicare and Medicaid Services (CMS) should pay for the nearly 10,000 procedural codes physicians use to charge for services. The RUC routinely overvalues specialist codes and undervalues primary care codes. Each year, CMS adopts the vast majority of those recommendations without changes. (Editor’s note: See Special Deal: The Shadowy Cartel of Doctors that Control Medicare by Haley Sweetland Edwards in the Washington Monthly, July 5, 2013.)
The result is a healthcare system focusing most of its resources on treating the very sick. Just 5 percent of payments go to preventing sickness, diagnosing diseases early, and helping the chronically ill, who consume an estimated 80 percent of all healthcare services, avoid more serious illness. These misplaced priorities are also responsible for America’s shortage of primary care physicians. Few medical students choose to jump on a primary care treadmill marked by 10-minute office visits when they can earn two to three times more by becoming a high-paid specialist, allowing most of them to pay off exorbitant loans.
Stat, the online publication that covers the healthcare industry, reported last month that advisers close to Kennedy put changing physician compensation on the former presidential candidate’s radar screen. They included Calley and Casey Means, wellness entrepreneurs and bestselling authors whose company, Levels, sells continuous glucose monitoring to the worried well. Casey Means is a surgeon who left her practice to become chief medical officer of the brother-and-sister’s start-up in 2019.

The two initially backed RFK’s short-circuited presidential campaign. After the election, Calley Means posted on X, “Our CMS codes embed a system that waits for Americans to get sick and profits. This is ground zero for driving better health outcomes and government efficiency.”
The Means siblings won right-wing adulation after appearing on Tucker Carlson’s show when Kennedy was still running as a third-party candidate. Just before the election, Joe Rogan interviewed them on his top-rated podcast. “After joining the Trump transition team, Kennedy shouted the Meanses out by name,” Stat reported, “saying in a public appearance that he would put people like them atop the nation’s health agencies if given his choice.” Casey has worked for Republicans, including the late Senator John McCain, and Calley told Bill Mahar on his HBO show that she’s not a Trumper.
If either takes a top post at CMS, they will face a formidable enemy in the AMA and the physicians whose specialties benefit from current pay scales. (Trump’s nominee to head CMS is Mehmet Oz, the author, celebrity, and physician who lost his U.S. Senate bid in Pennsylvania in 2022.) The AMA owns a copyright on physician payment codes.
While the AMA refuses to disclose the exact amount of royalties it receives from the use of payment codes in billing software, I estimate it to be at least $200 million annually. The non-profit’s most recent IRS filing shows the AMA reaped $269 million in total royalty revenue in 2022, a figure that excludes sales from publication subscriptions, reprints and educational materials, which are reported separately.
Conflicts of interest on the RUC
The medical profession justifies higher pay for specialists by claiming it takes more time, practice, and know-how to perform or manage complex procedures and cases. Specialists also undergo training programs that last anywhere from one to three years longer than primary care physicians.
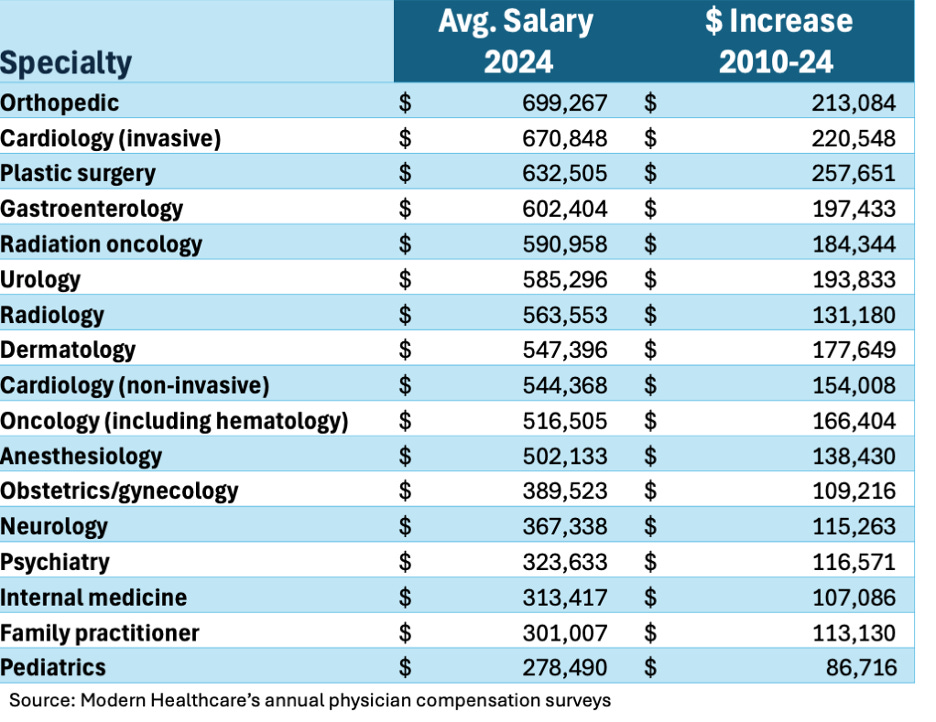
But critics point out that it’s a circular argument that fuels the self-interest of specialists. The AMA estimates time through surveys of physicians in each specialty conducted by the medical societies that sit on the AMA’s RUC. While the AMA insists it has taken steps to reduce the disparity in recent years, the spread between top specialist pay and primary care physician pay has grown wider (see chart).
Should the Trump administration, with or without a Secretary Kennedy, take on the RUC-AMA phalanx, they will face opposition from the GOP Doctor’s Caucus on Capitol Hill. Twenty of 26 medical professionals in Congress are physicians, and 19 belong to the GOP Doctor’s Caucus.
On the other hand, if a CMS under Dr. Oz takes on the current pricing scheme, he should find considerable support from liberals, who have pushed for physician pay reform for over a decade. As reported in the Washington Monthly in mid-2022, the prestigious National Academies of Science issued a report the previous year that called for raising investment in primary care to 10 percent of all health care expenditures, a doubling from current levels.
First efforts
Trump’s first administration did launch a few pilot projects to expand primary care pay. But Joe Biden’s administration was the first to attempt something systemic. CMS’s latest update of the physician pay scale, which agency officials estimated will lead to a 2.8 percent cut in overall physician pay, included new payment codes for primary care physicians. They can collect a flat monthly payment from CMS if they engage in activities coordinating care for their chronically ill patients.
“These efforts move us in the right direction, but we have a long way to go,” said Ann Greiner, president of the Primary Care Collaborative, a coalition of groups fighting for more significant funding for primary care. “We can’t just change how we pay. We have to change how much we pay. Pricing is an issue that must be addressed.”
The Trump administration could exploit modest cracks in the GOP Doctor’s Caucus. Senator Bill Cassidy, the Louisiana Republican and a physician, introduced the Pay PCPs Act along with his colleague, Sheldon Whitehouse, the Rhode Island Democrat. In addition to adding new hybrid payments for primary care that were included in the latest CMS rule, the bill would create “a new technical advisory committee to help CMS more accurately determine fee schedule rates.” However, Louisiana State Treasurer John Fleming has announced he will challenge Cassidy in the 2026 Republican primary because Cassidy voted to impeach Trump for his role in the January 6, 2021 insurrection.
The Urban Institute’s Robert Berenson, a physician and among the original architects of the fee-for-service physician fee schedule at CMS, called adjusting pay scales the key to deriving higher value and better outcomes from the current system. “If you pay a lot for certain procedures, you’re going to get a lot of those procedures. Other countries have improved value through adjusting the fee schedule,” he said.
Berenson has an idea that goes further than the Cassidy-Whitehouse effort. He wants legislation to establish an independent technical advisory panel that isn’t dependent on professional societies to determine how much their time and expertise are worth—a blatant conflict of interest in the AMA’s current setup. “If it’s done by CMS, it will be captured by the AMA,” he said. He’s right, and this is one place where Kennedy/Oz could do some good if confirmed.
A version of this story appeared first on the Washington Monthly website.
Merrill nails it again!
PCPs in other countries serve as gatekeepers to the consultants (specialists) and are better paid for their management of patients. The results are obvious every two years when the Commonwealth Fund compares the results across high-income countries. Since the comparisons began in 2004, the US has consistently ranked last.
It's time for the dinosaurs at the AMA to be replaced by an independent body that understands that illness prevention, chronic care management and dealing with the social determinants of health are key to Americans achieving the 4-5 year higher life expectancies of other high-income countries.
It is time for value-based compensation to replace the time-and-materials payment model like car mechanics. Primary care is also much more than gatekeepers to specialty care: they are managers, coordinating and orchestrating. That takes time that has no Relative Value Unit, but requires compensation if we want PCPs to truly manage cases and not just refer them on to higher paid specialists.
There is value in avoiding hospitalization and ER visits because preventive care and monitoring has been rendered. There is value in avoiding rebound hospitalizations and ER visits because post-discharge follow-up takes place in a timely manner. Tracking and focusing on medication adherence is another valuable primary care task. Can we agree that PCPs must be compensated for their time and expertise beyond transactional office visits?