


Raise hospital prices? In a pandemic?
It made sense in Maryland. Here’s why.

Late last spring, with non-essential surgeries at Greater Baltimore Medical Center on hold and its physicians’ practice nearly shut down, Dr. John Chessare, the 342-bed hospital’s chief executive officer, did what every economics textbook says he shouldn’t do when confronted by collapsing demand. He raised prices.
He wasn’t alone. Nearly every hospital in Maryland did the same thing.
When a brief research report about these actions appeared in JAMA in late January, my first reaction was disbelief. In recent years, hospitals have been under intense scrutiny for their pricing practices. A recent Rand report found privately insured patients across the country pay on average nearly 2 ½ times what Medicare shells out for the same service.
Kaiser Health News runs a monthly “bill of the month” feature where reporters investigate the causes of outrageous bills sent in by readers. President Joe Biden’s designee for Health and Human Services secretary, California Attorney General Xavier Becerra, earned his nod to become the nation’s top health care official by winning a major antitrust suit against Sutter Health, one of the most expensive hospital systems in the country.
But hospitals in Maryland are not paid like hospitals in other states and therein lies the story behind its price increases. Under its “all payer” system, privately insured patients pay the same price as Medicare and Medicaid for individual services. Waivers from the Centers for Medicare and Medicaid Services (CMS) dating from the late 1970s require the federal government to pay more than its usual fee schedule for Medicare and Medicaid patients, which in turn allows commercial insurers and self-insured private employers to pay less than peers in the rest of the country since they pay the same price as the government.
The state’s regulatory agency, the Health Services Cost Review Commission (HSCRC) and its staff of 50, sets uniform prices for each hospital, similar to the way state regulatory commissions oversee electricity and gas prices. Over the succeeding decades, Maryland hospital costs went from highest in the nation, about 25% above the national average, to about the national average, according to a 2015 Urban Institute report.
Global budgets: the latest wrinkle
In 2014 the state took the next major step in controlling hospital costs. It received another waiver from CMS that allowed HSCRC to set an annual global budget for each hospital in the state. The commission capped the budgets’ annual growth rate at about 3%, which is 40% less than the spending increases endured each year by public and private payers in most areas of the country.
The new regulatory scheme gave hospitals permission to adjust prices throughout the year to stay within their global budget. If demand rises more than expected, prices come down; if demand falls, prices go up. The state also established limits, called price corridors, on how much those prices could rise or fall in any given year. “All hospitals adjust our prices almost daily so we don’t go over the global budget,” Dr. Chessare said.
But when the pandemic nearly shut down discretionary operations, “we were given permission to extend the corridors to bill even more (to as much as a 20% increase). I see community hospitals in other parts of the country getting close to bankruptcy. But in Maryland, we are protected by the waiver and the HSCRC’s rules.”
There’s a catch, of course. Hospitals still must remain within their global budget, although the recoupment can be spread over several years. Since most hospitals also received CARES Act bailout money, prices will need to come down by a similar if not greater amount when volume returns. “The deal was we’re going to level this out,” said Joseph Antos, a scholar at the conservative American Enterprise Institute who sits on Maryland’s HSCRC board.
The new paper in JAMA evaluated the interim results. It found the state’s hospitals recouped about $450 million in lost revenue through higher prices from May to July last year, the period when discretionary physician visits and hospitals’ non-COVID stays dropped precipitously. In Maryland, total inpatient revenue fell just 1.6%; outpatient revenue fell only 15%. The decline in revenue nationally during that period was considerably higher.
“It pretty much worked in smoothing out the roughest edges of the first few months,” Antos said. “This is a mechanism that works best if the disaster is short term and isn’t that deep.”
This is just the latest evidence suggesting alternative payment models have proven their sea worthiness during the pandemic storm. Physician practices and hospital systems receiving prospective, monthly payments to provide all necessary services – so-called capitation – have also fared better financially during the pandemic.
Rapid adjustment of prices within a tightly regulated global budget provides the same incentives as capitation for eliminating useless tests and procedures, which a 2012 Institute of Medicine report estimated may be as high as 30% of all care. Unlike traditional fee-for-service medicine, where the easiest path for providers to make more money is to order more services, the guarantee of a global budget incentivizes Maryland hospitals to become more efficient and avoid unnecessary care. If they prescribe too many medically unnecessary tests and procedures or allow unnecessary admissions, it might send them over the cap.
No one has benefited more from the new system than private employers, whose employees’ use of hospitals fell significantly compared to peer hospitals during the first four years of global budgeting, according to a November 2019 report by RTI International. As the below chart shows, emergency room visits fell 2.6% compared to a similar group of hospitals in other states. Potentially avoidable admissions fell 6% even as admission severity fell, suggesting hospitals had become more willing to accept patients when attending physicians though it was necessary.
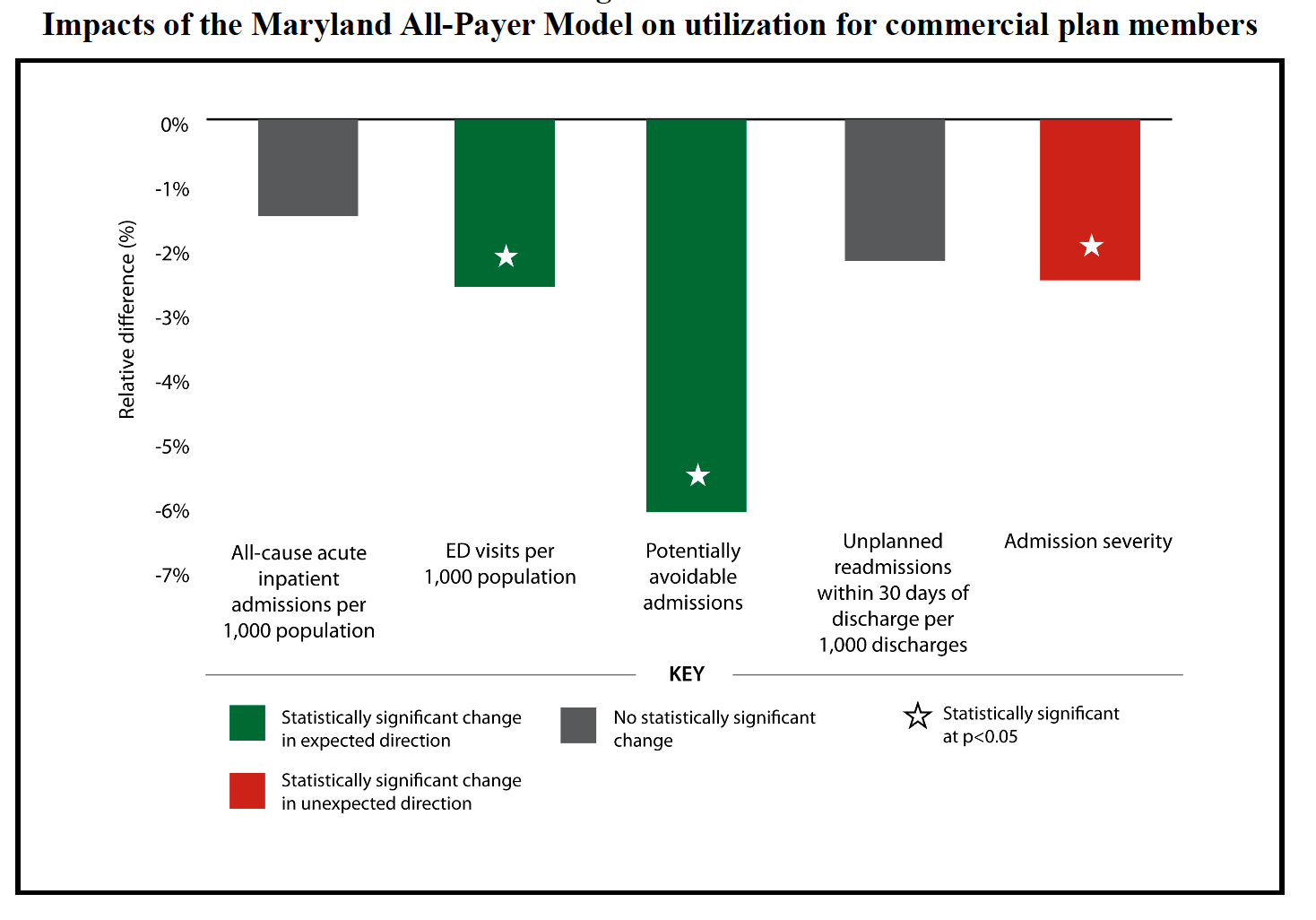
Source: RTI International, Evaluation of the Maryland All-Payer Model, November 2019
The higher prices that flowed from reduced utilization under global budgets has the ancillary benefit of providing unencumbered cash flow, which hospitals can channel into crucial services that are not reimbursed under fee-for-service. “Those of us who have drank the Kool-Aid are deploying the resources into patient centered medical homes, behavioral health and sexual assault forensic examination programs,” Dr. Chessare said. “We’re spending money in the outpatient area to drive better value.”
Patient advocacy groups often worry that global budgeting will force providers to stint on necessary care. Some point to the British National Health Service as an example of what can happen when governments ratchet down budgets, as has happened in Great Britain since the Conservatives took over the government in 2010. Public confidence in NHS fell from a peak of 70% a decade ago to 55% in 2019, though it has since recovered some of its luster during the pandemic.
I asked Katie Wunderlich, the executive director of the HSCRC, how Maryland has avoided that pitfall during its six-year experiment with global budgeting. “We do have quality metrics and measures on re-admissions that would make sure hospitals provide the right amount of care and appropriate care,” she said. “They’re not incentivized to withhold care altogether. There are checks and balances in place. Our goal is to reduce utilization overall such that it improves health outcomes and reduces the total costs.”
Still incomplete
Maryland’s all-payer/global budgeting system is far from perfect. It doesn’t encompass physician services, which consume about a third of the nation’s annual health care budget.
The state also faces a growing problem with high-paid specialists taking their procedures outside the hospital to avoid the budgetary limits. Ophthalmology, orthopedic and endoscopic physicians, in particular, have been moving discretionary, one-day procedures into stand-alone or hospital-owned ambulatory surgical centers, which are not covered by the global budget. Maryland has nearly twice as many ASCs per Medicare beneficiary as any other state, according to the 2019 Medicare Payment Advisory Commission report.

“When you have this constraint on one sector of the industry, you get this ballooning out on the other side,” said Robert Murray, who headed the HSCRC until 2011 and now consults with several other states contemplating all-payer schemes. “That is indeed one of the biggest challenges for the HSCRC now. They’ve done a reasonable job in reducing hospital costs, but there’s been this leakage to the non-hospital side.”
With the pandemic looking like it will drag on for at least another six months, the clamor for payment reform is growing. Last November, an influential group of health care thought leaders endorsed the Biden administration’s call for a public option to expand insurance coverage as long as it included capitation as its payment model. Medicare already uses capitation for its payments to private insurers selling Medicare Advantage plans, which now cover nearly 40% of all seniors in the program.
Both payers and providers have a lot to gain if politicians begin to take payment reform seriously. For providers, the capitation and all-payer/global budget models promise greater reliability in their revenue stream, which promotes staff stability. Hospitals across the country have shed hundreds of thousands of jobs during the pandemic. It also offers an exit ramp from the fee-for-service treadmill and its incentives to overprescribe unnecessary tests and procedures.
For organizations that ultimately pay the health care tab and endlessly fret about rising costs – that would be all employers, unions, state and local governments and patients/consumers paying ever higher out-of-pocket costs – both models offer a mechanism for long-term cost control. Growth rates under both are set by statute.
The politics of payment reform
I have never understood why the business community, which pays a third of the nation’s healthcare tab, refuses to put its considerable political clout behind far-reaching payment reform. Last month’s collapse of Haven, the ballyhooed joint venture between Amazon, Berkshire Hathaway and JPMorgan Chase that was set up three years ago to explore better ways to deliver higher quality care at lower cost, demonstrated the impoverished debate about health care taking place inside the nation’s C-suites.
The RTI analysis mentioned earlier evaluated who bore the burden of hospital spending under Maryland’s all-payer system by comparing all Maryland hospitals to a similar group of hospitals drawn from other states. The study found public payers in Maryland paid considerably more of the total tab while private payers paid considerably less. You’d think top-level executives would take note of that fact instead of leaving the burden of controlling their health care costs to the HR department.
Nor have consumer groups like Families USA and community-based health care organizations paid much attention to payment reform. Their main fight, of necessity, has been working to win universal coverage for low- and moderate-income Americans, who, for the most part, make up the 10% of the population that remains uninsured even when we’re at full employment. During the Trump years, health care advocates have also been distracted by the constant attacks on Medicaid at both the state and national level, which have cruelly restricted women’s access to reproductive health services and imposed destructive work requirements on the basic human right to adequate health insurance.
The single-payer movement, led by Vermont Sen. Bernie Sanders, has also eschewed taking on incremental payment reform at the state level, even though his Medicare for All bill, whose co-signers included now Vice President Kamala Harris, would establish a national budget for health care as its primary method for controlling costs. A single national plan would obviously be an all-payer plan since there would no longer be separate payment schedules for Medicare, Medicaid and private insurance plans.
I think that’s a strategic error on their part. By demonstrating that capitated payments or all-payer pricing tied to global budgets can work in states with different local economies and demographics, they would show a skeptical public that universal plans can solve the issue of rising costs. Before the pandemic hit, the 90% of Americans with health insurance said that was their top health care concern.
Success at exporting the Maryland model or a capitated payment model to a few more states would also show that hospitals and physician practices can adapt to global budgets. That would dramatically change the tenor of the national debate.
How to achieve universal coverage would no longer be the only question on the table, which perpetually skews the political debate toward addressing most peoples’ legitimate fear of losing what they have. Instead, we could begin debating how to properly regulate medical prices, budgets and insurance plans at the state level to achieve both universal coverage and cost control, and whether we need a national plan to get the job done.
That could be a single-payer plan run by the federal government. Or, as in Germany, it could be single-price system administered by highly regulated insurance companies, which could include integrated delivery networks like Kaiser Permanente or large physician practices that have the management skills and financial strength to take on the risk of operating under a fixed budget.
Either way, there would still be competition among providers and, if politicians chose the German route, among insurers. Only the competition would no longer be based on price. It would be based on quality, outcomes, efficiency and service – the things that people truly care about when it comes to health care. It’s only the current system that forces them to think first and foremost about the price, when what they’re really looking for is a helping hand.