
The silent epidemics
Soaring obesity, uncontrolled hypertension behind fast-growing Medicare spending on dialysis

Regular readers may wonder why I spend so little time writing about the pandemic. The answer is simple: When a third of Americans refuse to follow sensible public health guidelines, what purpose is served by my adding to the media cacophony castigating vaccine/mask skeptics and public health officialdom’s inadequate response?
Yesterday’s appointment of Dr. Ashish Jha as the new “pandemic czar” in the White House is a case in point. The dean of Brown University’s public health school has little government experience and none coordinating the complex and oftentimes competing government agencies responsible for public health. On the surface, Jha would seem a poor choice for coordinating the government-wide response to COVID-19, as an article in STAT pointed out this morning.
His predecessor Jeffrey Zients, while lacking medical experience, at least had the virtue of being a long-time government apparatchik who previously coordinated the U.S. response to the Ebola threat. Jha served on an advisory panel for that 2014 effort, but has since served mostly as a media talking head on public health issues.
For what it’s worth, I wish Jha well. Outsiders can sometimes serve as catalysts for change. Given the likehood of another COVID wave, here’s hoping his demonstrated communication skills can convince the third of the public that remains in thrall to rightwing media and demagogues to heed the call for another vaccine push or for renewed protective measures should they become necessary.
A different public health fiasco
I’m skeptical, which brings me to today’s topic. Public health pronouncements have had zero impact on the nation’s two largest public health disasters, which long predate COVID and are major drivers of rising health care costs, especially for the nation’s Medicare program. They are rising obesity, which is the leading cause of diabetes, chronic kidney disease and end-stage renal disease (ESRD) requiring dialysis; and uncontrolled high blood pressure (hypertension), which is the leading cause of heart attacks and strokes and the second leading cause of chronic kidney disease and ESRD.
A new report from the Centers for Disease Control and Prevention examines the health and financial toll taken by these twin epidemics through the prism of dialysis, the only condition covered by Medicare for the entire population. Diabetes accounts for 47% of new dialysis patients each year and uncontrolled hypertension accounts for another 29%.
Over the first two decades of this century, the number of chronic kidney disease patients who each year reach end-stage and require dialysis soared 42% to 131,423. The total number of people on dialysis more than doubled to nearly 800,000 (the average life expectancy for someone on dialysis is somewhere between 5 and 10 years).
On a populaton-adjusted basis, the annual new case rate went from 33 to 40 per 10,000 population. The total rate for people on dialysis soared from 127 to 238 per 10,000 population over the last two decades.
As a result, Medicare’s total tab for dialysis treatments soared 41% in just the past decade, reaching $49.2B in 2018. Even after adjusting for inflation, that’s an increase of more than 20%. Dialysis spending now accounts for nearly 1 in every 10 dollars spent by the Medicare program.
One final datapoint from the report: In 2000, diabetes and hypertension were the primary causes of 70% of patients entering dialysis and 60% of the total dialysis population. By 2019, those numbers had grown to 75% and 66%, respectively.
There’s no mystery as to why. Here are two maps showing the growth in state obesity rates over the past decade. First 2020 (the dark red shows obesity rates between 36% and 40% of the adult population):

Here’s the same map in 2011:
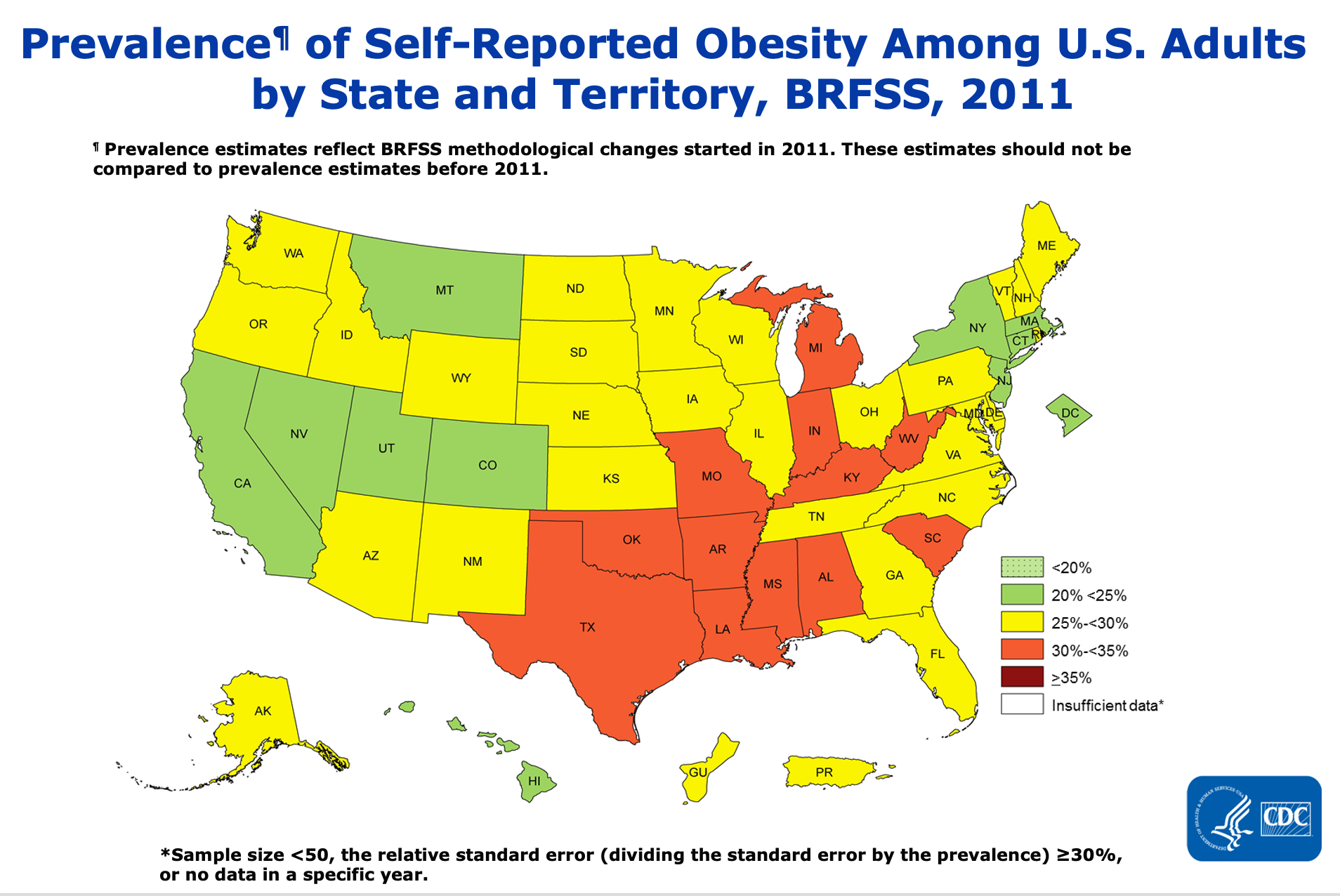
Overall, the prevalence of obesity in the general population soared from 30.5% in 2000 to 42.4%. Severe obesity now affects nearly 10% of the population, more than double the rate of two decades ago.
Uncontrolled high blood pressure
Since obesity is a major contributor to hypertension, its rate in the general population shows a similar upward trend. By 2018, nearly half the adult population had high blood pressure with 79% or 92 million people meeting the clinical practice criteria for prescribing medication. Unfortunately, 37% of that group remains untreated.
You would think public authorities in the U.S., not to mention Medicare’s fiscal watchdogs and assorted deficit hawks, would be jumping up and down over these frightening numbers. These twin, obesity-driven health crises represent a grave threat to the financial stability of the Medicare program.
Yet no one since Michelle Obama served as First Lady in the White House has used the bully pulpit to encourage Americans to improve their diets and exercise routinely. That’s the number one doctor-recommended approach for reducing weight and blood pressure.
And while there are sporadic efforts by the health care system to reach out to the 34 million Americans — disproportionately Black, Hispanic and Asian-American — whose high blood pressure is uncontrolled and untreated, no one in government has made it a priority.
During interviews with the press outlining his priorities yesterday, Health and Human Services Secretary Xavier Becerra said nothing about the ongoing public health crises facing America: Rising obesity rates; uncontrolled hypertension; substance abuse and gun violence chief among them.
There’s a good chance that over the next six months we will finally see COVID morphing from a society-disrupting pandemic to a manageable endemic disease, one whose cost in deaths, dollars and stress on the health care system will be comparable to the annual flu. In anticipation of that possibility, top health officials in the Biden administration should be preparing now for the public health system to pivot to addressing the long-term threats to our national health and well-being.