


Weekly research round-up
Where I read hidden gems in the medical literature so you don't have to

Shortchanging public health left states ill-equipped to deal with Covid-19
Our federal system gives primary responsibility for public health to state and local governments, which, as we all know, stumbled badly when the COVID-19 pandemic hit. No wonder. As a nation, the U.S. spends just 2.5 cents on public health for every dollar it spends on caring for the sick.
A new study in Health Affairs reveals those misplaced priorities grew worse in the past decade. Average spending on public health fell 5.7% to just $76 per person in the decade leading up to 2018. Categories with major declines in spending included maternal and child health (down 21%) and environmental health (down 36%). Only injury prevention – the smallest category – showed an increase over the decade. State and local governments spend a paltry $1.90 per capita per year on pandemic preparedness. The COVID-19 pandemic cost the average American family about $50,000 in addition to the over half million deaths and ongoing medical obligations to the millions with lingering aftereffects from the illness.
This new study contradicts the generally positive outlook on public health spending given each year by the Centers for Medicare and Medicaid Services (CMS), which claims average spending grew 23% over the decade. The studies authors, led by researchers at the Johns Hopkins University Bloomberg School of Public Health, argue that by failing to count spending by non-health agencies (environment, agriculture and housing departments, for instance), CMS “substantially overinflates actual spending on government public health.”
The Affordable Care Act included a large boost for public health through its Prevention and Public Health Fund. But the Obama administration, hamstrung by a Republican Congress after 2010, raided the fund to pay for ads and other measures that encouraged people to sign up for insurance on the exchanges. The Trump administration took that one step further by robbing the fund to pay for health care delivery while, at the same time, dismantling the pandemic preparedness office.
No doubt, when new data is available, post-pandemic spending on public health will show a sharp increase since last year’s CURES Act and the more recent American Rescue Plan included substantial boosts for state and local health agencies. The study’s authors categorize this as the traditional U.S. approach to public health: “neglect, panic, repeat.”
Medicare Advantage: No advantage in reducing unnecessary care …
Estimates of unnecessary or “low value” care, defined as services that provide little or no clinical benefit, range from 10% to 30% of all health care spending. Seniors on Medicare are especially prone to receiving tests, procedures, images and medications that are more likely to cause harm than good. In 2012, the ABIM (American Board of Internal Medicine) Foundation launched a “Choosing Wisely” campaign to encourage medical professional societies to identify practices that ought to be eliminated or sharply curtailed.
It stands to reason that Medicare Advantage insurers, which receive a lump sum for every beneficiary whose choose their plans, would have a major interest in eliminating unnecessary care. Every dollar they don’t have to spend on providing health care services either falls to their bottom line or can be spent on providing services like dental and eyeglass coverage that aren’t covered by traditional Medicare.
Yet a new study in JAMA Internal Medicine found there was essentially no difference in use of low-value services in Medicare Advantage programs compared to seniors who remain in the traditional fee-for-service Medicare program. The researchers also discovered neither group showed a decline in unnecessary care with the sole exception of cancer screening in the very old, which fell in both groups.
The authors offer a variety of possible explanations for why MA plans failed to reduce unnecessary care. Most such services are relatively low-cost, thus the potential for savings is low, they noted. Plans are more interested in raising their quality scores, which helps them attract more customers. And physicians working for MA plans are still on fee-for-service reimbursement, which means eliminating unnecessary services reduces their income.
Indeed, use of low-value services was actually higher for individuals enrolled in MA plans, although the differences weren’t statistically significant. CMS should “reconsider the design of financial incentives in the traditional Medicare and Medicare Advantage programs,” the authors concluded.
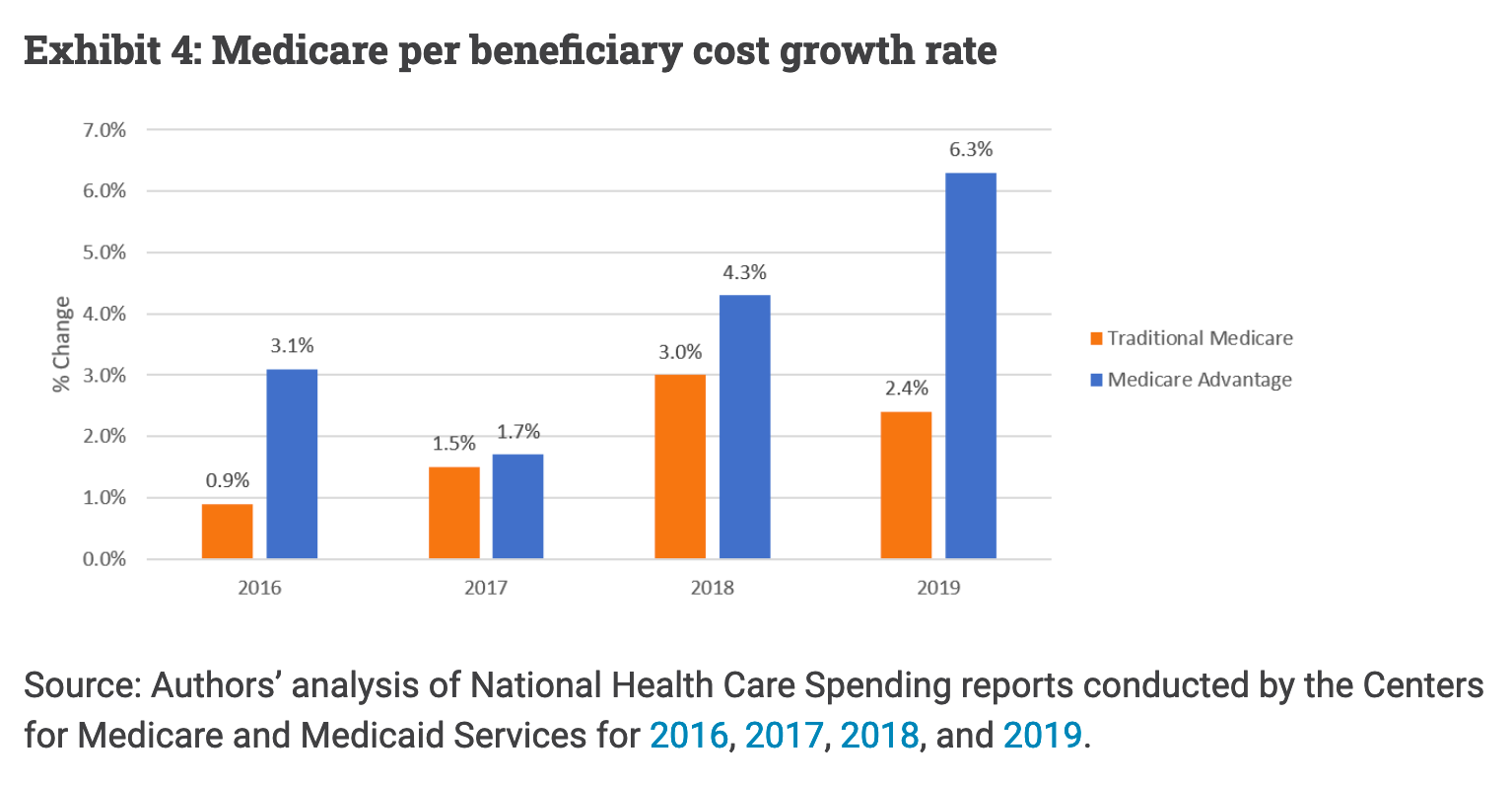
… And its costs are rising faster than traditional Medicare
In 2019, Medicare Advantage cost-per-enrollee soared 6.3% compared to just 2.4% for fee-for-service Medicare. It was the fourth year in a row that its cost growth exceeded the traditional program, according to a recent blog post on the Health Affairs website.
That’s odd, the authors note, since CMS is already paying MA plans more than the average cost of care for beneficiaries in the traditional program (101% to 104%, according to a recent Medicare Payment Advisory Commission report). Moreover, the average pretax margin for MA plans is 5.2%, and, according to health insurers, MA plans spend 20% to 40% less on care than traditional Medicare.
Is that because MA plans pay providers less, skimp on care or improve the care coordination that reduces preventable hospitalizations? “We don’t know,” journalist Ken Terry and Leavitt Partners consultant David Muhlestein write.
Is coding intensity the culprit for rising MA costs?
The most obvious explanation for Medicare Advantage’s rising costs is plans’ well-known tactic of raising beneficiaries’ risk profile (and thus reimbursement per beneficiary) by combing through medical records to find diagnoses that aren’t being treated. A simple example is finding a patient whose cholesterol level is slightly elevated, but isn’t on a statin.
It’s known as “coding intensity.” A recent study in the journal Health Services Research took a look at where this extra money goes. They found for every $1 in revenue from coding intensity, 21 to 45 cents went to increasing plan profitability; 10 to 19 cents went to reducing plan costs to the government; and 11 to 16 cents went to reducing premiums for beneficiaries. “While coding intensity increases taxpayers’ cost of the MA program, enrollees and plans both benefit but with larger gains for the plans,” the authors concluded.
In its latest report on the MA program, the Medicare Payment Advisory Commission notes that 43% of seniors are now in Medicare Advantage plans – a record high. MA insurers’ average spending level on services are just 87% of the traditional program, despite receiving slightly more revenue from the program. When asked in a recent briefing to compare quality in the two approaches to delivering Medicare benefits, executive director James Mathews said “we can’t say anything about the quality of care. We need to overhaul the quality bonus program.”